
In the past, serious ACL injuries would have put a stop to sporting careers, however now with the advancement of rehabilitation and surgical practices, most people recover quicker and are able to continue in their chosen sport for a much longer period of time.
THE ANATOMY OF THE KNEE
The knee itself is a very complex joint in the body.
It is a hinge joint, therefore is structured to perform 2 principal actions of flexion (to bend) and extension (to straighten). The knee is provided support and stability, from the quadriceps muscle for extension and the hamstrings for flexion and the following ligaments –
- Anterior Cruciate (ACL)
- Posterior Cruciate (PCL)
- Medial Collateral Ligament (MCL)
- Lateral Collateral Ligaments (LCL)

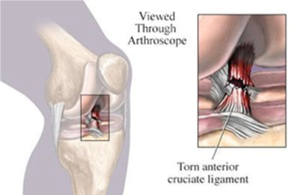
WHAT IS AN ANTERIOR CRUCIATE LIGAMENT?
Your cruciate ligaments are inside your knee joint. They cross each other and form an ‘X’, with the PCL at the back and ACL at the front. These ligaments are essential stabilising structures of the knee and control the way your knee moves back and forth.
The ACL, specifically, allows for rotational movement like twisting, turning and sidestepping. It prevents the tibia from moving forwards when weight bearing and prevents rotation of the joint.
WHAT IS AN ACL TEAR CAUSED FROM AND WHO IS MOST AT RISK?
An ACL tear is most likely caused from a sports related injury, as they occur when pivoting, changing direction quickly, landing from a jump, or stopping suddenly.
However they can sometimes occur from rough play, falls, car accidents or from work injuries.
Half of all injuries to the ACL coincide with damage to other structures in the knee, like articular cartilage, meniscus or other ligaments. Unfortunately, the ACL cannot repair itself naturally, so the knee often becomes unstable and gives way, and in the long term it can lead to arthritis or acute meniscus tears.
Due to differences in physical conditioning, neuromuscular control and muscular strength, studies have shown that females have a higher risk of ACL injury than males in some sports. This may also be caused by different leg and pelvis alignment, looseness of ligaments and oestrogen effects on ligaments.
WHAT ARE THE SIGNS OR SYMPTOMS OF AN ACL TEAR?
 Often people hear a ‘popping’ or ‘cracking’ noise when they have a severe ACL tear or injury. Their knee will give way from under them and they will feel extreme pain.
Often people hear a ‘popping’ or ‘cracking’ noise when they have a severe ACL tear or injury. Their knee will give way from under them and they will feel extreme pain.
Other symptoms are –
- Pain and swelling
- Soreness on joint line
- Loss of range of motion, especially extension
- Pain when walking
HOW IS IT DIAGNOSED?
It is very important to see a sports medicine professional as soon as possible after the injury. They may perform a physical exam and take x-rays of the knee to determine the extent of the injury and provide advice for treatment. Presenting for an exam within the first hour, is often beneficial before hemarthrosis (bleeding into the joint) develops and significant swelling sets in. An MRI test may also be recommended to confirm a diagnosis.
IMMEDIATE PAIN MANAGEMENT
The initial treatment of the injury is the same as any soft tissue injury. This consists of the RICE protocol which should be completed for the first 48-72 hrs. This will reduce the bleeding and damage to the joint. The RICE method is as follows –
- Rest
- Ice
- Compression
- Elevation
The knee should be rested in a raised position and an ice pack applied for 20 mins every 2 hours. A compression bandage can be applied to limit swelling and bleeding further.
WHAT ARE THE TREATMENT OPTIONS?
Treatment will vary depending on the patient’s individual case and needs. These may include –
- The degree of instability
- The age of athlete
- The type of sport played by athlete
- Expected demands to be placed on the knee
- Other associated injuries
- Social issues like costs and time off work
For those not looking to re-enter their chosen sport, who perhaps are elderly or have a low activity level, a non-surgical treatment option may be effective. As long as the knee is stable, you may be recommended bracing or physiotherapy only. Even for athletes, non-surgical management can be as successful with a thorough rehabilitation program.
Initially, bracing will protect the knee from further instability, along with the use of crutches.
Physiotherapy will be a part of all rehabilitation, whether surgery is required or not. They will provide specific exercises to restore knee function and strengthen the muscles surrounding the joint.
Surgical reconstruction is also a common method to repair a torn ACL. It is generally considered after the initial 4-6 week period after the injury, to allow for inflammation and pain to settle.
Unfortunately, most ACL tears can’t be sutured back together so the ligament must be reconstructed using another tendon or ligament. The surgeon will replace the torn ligament with a tissue graft which can be obtained from various sources, such as harvested from the patellar tendon, hamstring, or quadricep tendon.
In general this surgery is very successful. Whilst it won’t provide you with a normal knee again, it will make it more stable.
Like with any surgery however, there are risks to consider. These include- infection, stiffness, ongoing instability and pain, and difficulty returning to previous level of sport.

REHABILITATION OF AN ACL INJURY
Rehabilitation plays a very important role in getting you back to your normal routine and often the sooner you can start the better.
Rehabilitation will usually be managed by a Physiotherapist, should surgery not be required. Otherwise they will work under the direction of the orthopaedic surgeon, after surgery.
There are a number of rehabilitation programs, however generally they will include a program of protected mobilisation, then strengthening activities and functional exercises. The overall aim will be to restore motion and strength and improve knee stability to prevent future injuries. It is very important that you listen to your body and health professional, and you progress as your body allows. Forcing a quicker recovery, or taking it too slowly, may be detrimental to your overall recovery.
Rehabilitation after surgery generally takes between 6 and 9 months. After strength, range of motion and coordination are almost at full capacity, the orthopaedic surgeon or physiotherapist will be able to provide approval for the athlete to return to their chosen sport.
REHABILITATION WITH THE TEAM AT SPHC
Sandgate Physical Health Clinic have highly qualified and experienced Physiotherapists to assist you with diagnosing your ACL injury, further assessment as required and ongoing rehabilitation to get you back to full recovery, as soon as possible.
Call today to arrange an appointment on 07 3869 1099 or BOOK ONLINE.